
How to Read Your AR Aging Report (And What to Do When the Numbers Are Off)
You run the AR aging report. A spreadsheet of numbers stares back at you. Some of it looks fine. Some of it looks... not fine. But what does "fine" actually mean, and what should you actually do about the rest?
The aging report is one of the most useful tools in behavioral health billing, but only if you know how to read it. Most guides treat it as a generic medical billing topic. This one is written for behavioral health practices specifically — because your payer mix, your programs, and your timelines are not the same as a primary care clinic.
Here's what each part of the report means, what the numbers should look like, and how to take action when your buckets are heading in the wrong direction.
What Is an AR Aging Report, and Why Does It Matter?
An AR aging report is a snapshot of every unpaid claim and client balance your practice is carrying, sorted by how long each has been outstanding since the date of service.
It has two distinct parts: insurance A/R (what payers owe you) and patient A/R (what clients owe you). These behave differently and require completely different follow-up. Treat them separately in any analysis.
Why does this report matter? It's the clearest window into your revenue cycle health. A well-managed accounts receivable aging report means predictable cash flow. A neglected one means revenue quietly leaving the practice while you're focused on your clients.
Think of it as an early warning system. The problems showing up in this report today are the cash flow problems you'll feel in 60 to 90 days. A 6-provider outpatient behavioral health practice in the Twin Cities that hasn't reviewed their aging report in two months might find that 28% of their A/R is sitting past 90 days. That's almost always the first sign that claim follow-up has broken down somewhere.
How to Read the Aging Buckets
The standard aging buckets in medical billing are 0–30 days, 31–60 days, 61–90 days, 91–120 days, and 120+ days. Each one tells you something different and calls for a different response.
0–30 days: Normal. Claims are in process. No action needed yet.
31–60 days: Time for a status check. Confirm the payer received the claim. Watch for soft denials or requests for additional documentation you may have missed.
61–90 days: Red flag. Something is stuck, whether it's a denial, missing information, or a payer processing backlog. These claims need immediate attention, and so does your calendar. Some payers have a 60-day timely filing deadline, meaning the appeal window may already be closing. Know which payers that applies to before you start working the claim.
90+ days: Critical. Every day in this bucket risks crossing timely filing deadlines and eventual write-off. Escalate and work these claims urgently.
Keep insurance aging and patient aging separate when you analyze. A client who owes a $40 copay needs a statement sent. A payer sitting on a $1,200 claim needs a follow-up call. Different problems, different workflows, different urgency.
An ARMHS billing coordinator reviewing the 61–90 day bucket might find 14 claims concentrated with a single managed care organization. A closer look reveals the payer updated their prior authorization requirements three months ago — and no one caught it. Working those claims immediately, before they cross into the 90+ range, can save a significant chunk of recoverable revenue. This is exactly where denial tracking discipline pays off.
What the Numbers Should Look Like
Here's what a healthy accounts receivable aging distribution looks like, based on industry benchmarks:[1]
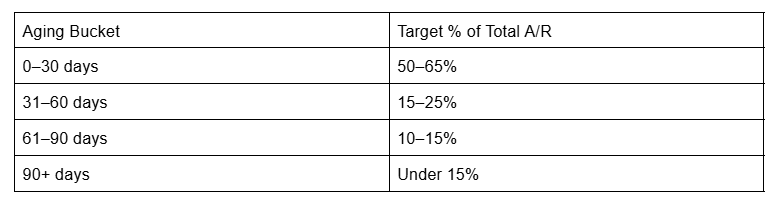
The goal for days in A/R is 30–40 days on average from date of service to payment.[2] Bad debt should stay under 3–5% of total charges.
Here's the important behavioral health caveat: don't benchmark yourself against general medical practices. Programs like ARMHS, CTSS, and Targeted Case Management have longer processing timelines than commercial outpatient billing. Documentation requirements are heavier. Medicaid processing runs slower. A practice billing primarily CTSS and ARMHS services may run at 38–42 days in A/R on average — technically outside the generic benchmark, but within normal range for their payer mix.
Knowing that difference prevents unnecessary alarm. It also prevents switching billing strategies for the wrong reason.
Compare your numbers to your own prior months before comparing to industry averages. Is your 90+ bucket growing month over month? That matters more than whether your Days in A/R matches a number designed for a primary care practice.
At BreezyBilling, we review A/R trends in monthly check-ins alongside each practice rather than just handing over a number. Context is what makes the data useful.
Warning Signs in Your AR Aging Report
Some patterns in the aging report deserve immediate attention, no matter what your overall numbers look like.
A growing 90+ bucket. If this bucket is larger month over month, claim follow-up has broken down somewhere. It won't correct itself.
Single-payer concentration in aged A/R. When one payer makes up a disproportionate share of the 61–90+ day balances, that's a systemic issue with that payer, not random variation. It needs a targeted response.
Timely filing exposure. Behavioral health Medicaid payers in Minnesota, including MHCP managed care organizations, have strict timely filing windows. Claims sitting near those deadlines need immediate escalation before the revenue is permanently lost.
Patient A/R stagnation. Client balances sitting unpaid for 90+ days often mean statements haven't gone out or client communication has lapsed. It's a different kind of leakage than insurance A/R, but it compounds quickly. Once a client gets a large balance it becomes significantly harder to get fully paid - even with a payment plan.
High write-off rate. Writing off claims without working them first is a sign the billing workflow is overwhelmed. Write-offs should be a last resort after denial follow-up, not a default response.
A solo therapist in Minneapolis once noticed her 90+ bucket had nearly doubled over three months. She pulled claim-level detail and found a pattern: a commercial payer had changed their portal submission requirements, and multiple claims were rejected without clear notification. Several months of legitimate claims were stuck, but workable — because timely filing hadn't run out yet. That's the kind of trend BreezyBilling's monthly A/R audit is designed to catch before it compounds.
A Practical Action Plan for Aged A/R
When the numbers are off, here's where to start.
Work the 61–90 day bucket first. This is your highest-impact, highest-recoverability category. These claims can still be saved. Work them before they tip into the 90+ range.
Drill down by payer, not just by bucket. Totals hide patterns. Sort the 61–90 day bucket by payer to find concentration issues. One slow payer can make your overall numbers look far worse than they actually are.
Set a review cadence and hold it. Weekly is best practice for most practices. Biweekly is a realistic minimum. Monthly is better than never, but it's not enough. Don't wait until cash flow hurts to open the report.
Work denials before they age. Denied claims in the 31–60 day range are the fastest path to recovered revenue. Identify the denial reason, correct the claim, and resubmit. Most denials are fixable if caught early — an AR cleanup project on an aged bucket is far more labor-intensive than staying current.
Turn the report into a workflow. For each aged claim you identify, note the issue, the action taken, and a follow-up date. This converts a passive report into an active collections tool.
Don't write off without working first. Before writing anything off, confirm the timely filing window hasn't closed. If there's still time, the claim is worth pursuing.
A clinic administrator at a 10-provider group practice in Rochester implements a biweekly aging review. In the first review cycle, they identify $9,200 in claims sitting in the 61–90 day bucket — most due to a missing authorization number that's easy to correct. They resubmit, and the majority of those claims pay within 30 days.
BreezyBilling's monthly performance check-ins create exactly this kind of accountability. Your account coordinator reviews the aging report with you, flags what's trending the wrong direction, and assigns action items. The aging report stops being a stress point and becomes a managed process.
Final Thoughts
The AR aging report isn't a scary document. It's a diagnostic tool that tells you exactly where your revenue cycle is working and where it isn't.
The problem is rarely the report itself. It's reviewing it inconsistently, not knowing what to look for, and not having a clear action plan when the numbers slip. For clinicians running behavioral health practices, billing complexity shouldn't be what keeps the practice from sustaining itself.
At BreezyBilling, every client gets a monthly A/R audit included as a core part of our service. Your dedicated account coordinator reviews the aging report with you, explains what's trending, and takes action. You don't interpret these numbers alone.
If your aging report has been sitting unread — or you're looking at it and not sure what to do next — we're happy to walk through it with you.
---
Sources
MGMA DataDive Provider Compensation and Production — Medical Group Management Association, 2024
A/R Aging in Medical Billing: Benchmarks and Best Practices — HCMS, 2024